Immune cell declines caused by islatravir are dose-related and reversible
At the International Congress on Drug Therapy in HIV Infection (HIV Glasgow) last week, the drug company MSD (known as Merck in the US) presented the first detailed data on the unexpected side effects of its new anti-HIV drug, islatravir.
Islatravir is a drug of a new class called nucleoside reverse transcriptase translocation inhibitors (NRTTIs). It was expected to be both resistance-proof and extremely persistent in the body, allowing for monthly oral dosing and six-monthly or yearly dosing with an injection or implant.
However, clinical development was paused last November when the drug was found to be associated with falls in many types of immune-system cells, including all lymphocytes (white blood cells), the B-cells that make antibodies, the NK-cells, and the T-cells, both CD8s and CD4s, that regulate cellular immunity and that are attacked by HIV.
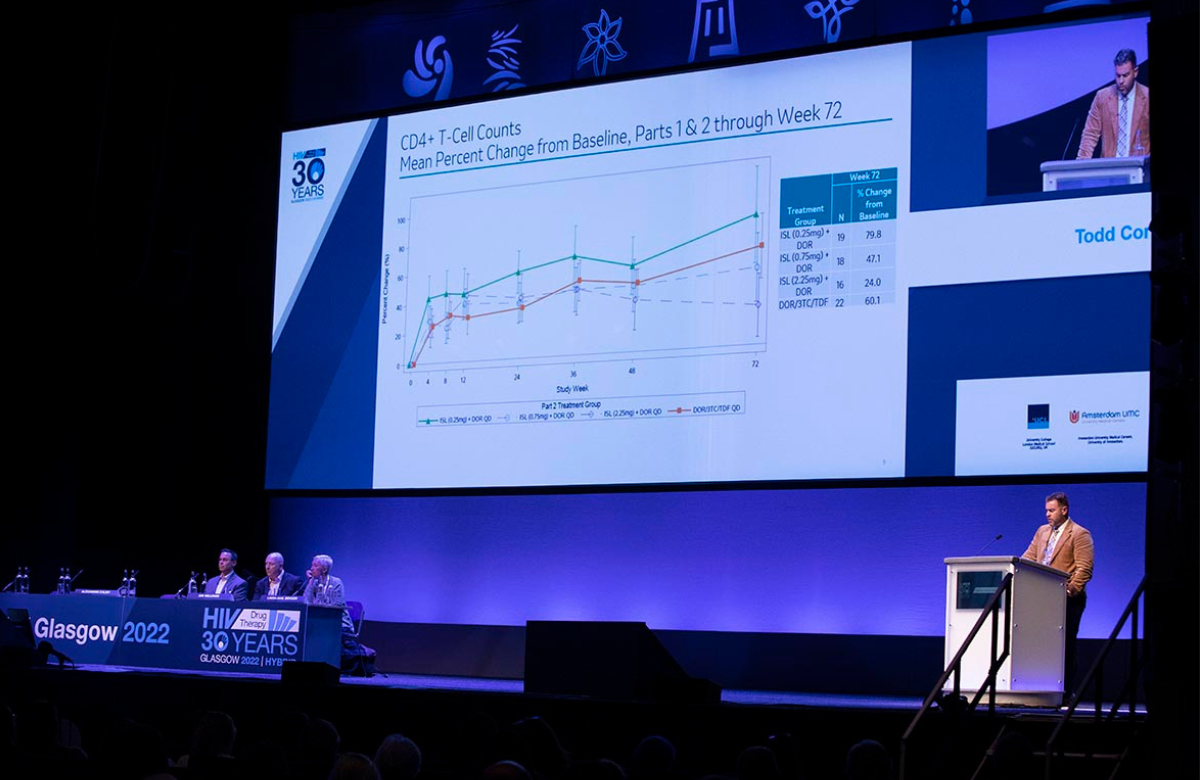
Todd Correll of Merck focused on data from a dose-finding phase II study, which included daily 0.25mg, 0.75mg and 2.25mg doses, plus a control arm not containing it. All were combined with doravirine and lamivudine.
The study allows a closer look at how the lymphocyte suppression varied with dose. For example, at week 72, total lymphocyte counts had increased by 20.5% from baseline in people on the lowest dose of islatravir and by 16% in people in the tenofovir arm. But they decreased slightly, by 0.4%, in people on 0.75mg islatravir and considerably, by 16%, in people on 2.25mg.
Because participants in two of the study arms changed doses, the findings also show whether the effects seen on larger doses were reversible. To generalise, if people switched from 2.25mg to 0.75mg islatravir, then their total lymphocyte, CD4 and B-cell counts went up; if they switched from 0.25mg to 0.75mg islatravir, they went down; and if they remained on 0.75mg, they stayed about the same.
MSD says that the lowest effective dose of 0.25mg should not produce significant declines in lymphocytes. This dose is therefore being taken forward in studies of daily islatravir and doravirine for treatment.
However, the larger doses and novel formulations of islatravir that held out the promise of monthly or even yearly dosing – and of a revolution in HIV prevention – won’t now be developed.
Rapid scale-up of PrEP in Ukraine this year

More than half the people on PrEP in Ukraine started it this year, and the country is hoping to further develop its PrEP services, Anna Koval of the Public Health Center of the Ministry of Health of Ukraine told the conference.
This is a remarkable achievement in a country where HIV clinics have been damaged or destroyed, much of the population is on the move, and many medical staff have been redeployed or relocated due to the war. Of the 250 medical facilities that could dispense PrEP before the war, 31 have now been destroyed, damaged beyond repair, or are behind Russian lines.
The continued expansion of PrEP, Koval said, has been possible only because of the partnership of community and non-governmental organisations, who have taken over most HIV testing and referral work, freeing medical staff solely to prescribe PrEP.
There were about 500 PrEP initiations per month in the period leading up to the war. Numbers fell dramatically immediately after the invasion at the end of February, but June had 732 PrEP initiations – the largest number ever seen. Currently, there are over 8700 people on PrEP in Ukraine, of whom 4559 started it in 2022.
“We want to further decentralise, to prescribe PrEP outside hospitals, and to implement more self-testing and telemedicine,” Koval said. “We still plan for a future, but our plans need to be mobile, because our situation is.”
Fewer Ukrainian refugees with HIV in Poland than expected

The number of refugees with HIV coming from Ukraine to Poland has raised the number receiving HIV care in Poland by 16%, Dr Miłosz Parczewski, President of the Polish AIDS Society, told the conference. This is fewer than expected. Ukraine has nearly ten times as many people living with HIV as neighbouring Poland – the leading host country for refugees from the invasion.
This could be for several reasons. Some refugees do not plan to stay in Poland and may be on route to other countries where their refugee status has been accepted; some people may have disengaged from care; and some refugees have sought care at peripheral hospitals in eastern Poland that have not yet provided data.
The different demographics and needs of Ukrainian refugees are making new demands on Polish services. For example, 80% of people living with HIV in Poland are men who have sex with men. Ukraine’s HIV epidemic, on the other hand, having started in people who inject drugs, is now dominated by heterosexually acquired infections. The number of vertically infected children receiving HIV treatment in Poland has almost doubled in a few months.
One issue doctors have had to deal with is that the combination pill taken by the majority of Ukrainians living with HIV is not available in Poland, so many patients have needed to switch treatment. Another concern is that many Ukrainians have an HIV subtype called A6 which is rarely seen in other European countries. While there have been questions about whether resistance to HIV drugs, especially integrase inhibitors, may develop more frequently with this subtype, the news so far is reassuring.
Re-suppression of HIV after viral rebound

Dolutegravir-based treatment is significantly more likely to result in re-suppression of HIV after viral rebound than treatment containing efavirenz, a meta-analysis of four large clinical trials has reported.
The capacity of an antiretroviral regimen to re-suppress HIV after viral rebound is an especially important question for lower- and middle-income settings where a limited number of regimens are available. If first-line treatment fails, second-line treatment is considerably more expensive, so it is critical to understand the likelihood of viral re-suppression when people continue with their existing regimen and receive enhanced adherence counselling, in line with World Health Organization guidelines.
Dr Andrew Hill and colleagues pooled data from four large studies that compared dolutegravir to efavirenz-based or protease inhibitor-based treatment in sub-Saharan Africa. In the meta-analysis, viral re-suppression rates in participants who had experienced viral failure (a viral load above 1000) and did not change treatment was significantly higher for dolutegravir than efavirenz (p=0.04).
Dr Hill said that more research was needed to assess how much adherence counselling and sustained viraemia are required before people taking dolutegravir are offered a new regimen. He pointed out that new South African treatment guidelines only recommend a switch from dolutegravir if integrase inhibitor resistance is detected.
Injectable HIV treatment in practice

Early German data from patients taking injectable cabotegravir and rilpivirine (Vocabria/Rekambys in Europe, Cabenuva in North America and Australia) in a demonstration project, shows that patient dissatisfaction with taking antiretroviral therapy (ART) halved after six months’ experience. During this time, 89.5% of participants remained on the therapy and with a viral load below 50 copies.
Only two of 236 people taking cabotegravir/rilpivirine had virological failure, defined as two consecutive viral loads over 200. One of the two patients with virological failure should have never been in the study, because it was found afterwards that a previous regimen containing NNRTI drugs had failed, leading them to develop resistance to rilpivirine. But the other is puzzling, as they had no apparent risk factors.
A separate analysis clarified the risk factors for virological failure of cabotegravir/rilpivirine. The analysis included data from 1363 people who took part in three clinical trials, with some participants having now taken the injections for three years. The pooled rate of viral failure was 1.4% or 0.54 per 100 person-years of follow-up.
Three baseline factors emerged as significant predictors of viral failure: the presence of rilpivirine resistant mutations, HIV-1 A6 or A1 subtype (mostly found in Russia and neighbouring countries) and greater body mass index.
A combination of two factors was strongly associated with virological failure (treatment failed in 19% of people with two risk factors). Virological failure was much less common in people with a single risk factor (2.0%) or no risk factors (0.4%).
However, identifying rilpivirine resistance is challenging for clinicians. People who are virally suppressed cannot have their viral RNA sequenced for a resistance test. It is possible to sequence proviral DNA, but this is expensive, and most clinics don’t do it. The only alternative is to rely on clinical history (previous failure of drugs from the NNRTI class), but this information is not always available.
Pregnancies in women born with HIV

An increasing number of women who grew up with HIV are now having their own children, UK researchers told the conference. Between 2006 and 2021, there were 17,478 pregnancies in women living with HIV in the UK, including 202 pregnancies in 131 women who grew up with HIV. During this time period, the proportion of mothers who grew up with HIV increased from 0.3% to 3.5%.
Pregnant women who grew up with HIV were significantly younger (median age 24) than pregnant women who probably acquired HIV through heterosexual sex (median age 33). Although more women who grew up with HIV were accessing HIV treatment at the time of conception, rates of viral suppression were slightly lower than for women who acquired HIV later in life.
Outcomes in both groups were broadly similar, but there was an increased risk of preterm births and low birth weight babies in women who grew up with HIV. Of the 150 babies born to women growing up with HIV with complete follow-up, one was diagnosed HIV positive.
Cardiovascular disease and prevention

Almost half of a large European cohort of people with HIV were at very high risk of cardiovascular disease, but a substantial proportion were not receiving preventive medication, HIV Glasgow was told.
The study examined data from 22,050 people living with HIV in Europe and Australia between 2012 and 2019.
A very high risk was defined as a 10% or greater risk within ten years of a serious cardiovascular event such as heart attack, stroke or death from a serious cardiovascular event, or surgery for major heart disease. The proportion with very high risk of heart disease rose from 31% in 2012 to 49% in 2019.
However, one third of people eligible for medication to reduce their blood pressure were not receiving it in 2019 and 43% were not receiving medication to reduce lipid levels. A similar proportion were not receiving medication to control their blood sugar.
Gay and bisexual migrants in France

In France, gay and bisexual men born abroad have higher prevalence of HIV, a higher rate of new infections, and are more likely to remain undiagnosed. They are also highly concentrated in the Paris region.
New data presented at the conference showed that at least 38% of this group had acquired HIV after moving to France. HIV acquisition after arrival in France was more common in men from north Africa (73%), Asia and Oceania (61%) and sub-Saharan Africa (53%) than in men from Europe (47%) or Latin America and the Caribbean (39%).
The study findings highlight a high level of HIV prevention and social need among gay and bisexual men migrating to France.
Simple scoring system predicts survival

A scoring system that can identify which older people with HIV have a poorer prognosis is just as accurate in Swiss people with HIV as in the French population, the conference heard.
The Dat’AIDS score was developed by looking at mortality in people with HIV over the age of 60 living in France. Eight factors were associated with the risk of death: age, CD4 count, non-HIV related cancer, cardiovascular disease, kidney function, liver cirrhosis, low body mass index and anaemia.
The new study validated the score with members of the Swiss HIV Cohort. The outcomes predicted by the scoring system showed very good concordance with observed mortality.
Identifying which people with HIV have a higher risk of poor survival is important for prioritising clinical interventions. The scoring system can also provide reassurance to those with lower scores.