Gay men and fatherhood

HIV clinicians should ask gay and bisexual men if they want to become fathers and share information about how that would be possible, researchers say. They talked to both healthcare professionals and gay men living with HIV in London, and found that discussions about parenting were rarely initiated by either side.
Just under half of the gay men living with HIV who were interviewed for this small study said they might be interested in becoming a parent. For some men, it was one of the first questions they had after being diagnosed with HIV, but other men had simply assumed that the virus made it impossible to have a child.
Options for gay and bisexual men include adoption, fostering, having a child with a surrogate mother (i.e. using self-insemination, artificial insemination or egg donation) and co-parenting (conceiving and raising a child with a female friend or couple).
However, not all men in the study were aware of these possibilities, or understood the circumstances in which HIV may (or may not) be passed from a parent to child. An undetectable viral load prevents transmission – and HIV can’t be passed directly from the biological father to the baby anyway.
Men said that they would have liked to have been told that having a child was a possibility, partly because of what it symbolises. It would have been good to know when they were diagnosed, some suggested.
As one man said, “It’s that whole thing when you’re diagnosed – you do question the future… Even if I wasn’t interested [in having children], the very fact that someone could come and tell you, well, you can still be a parent, means that you actually then think, oh, well, then I can live much longer if you think I can be a parent.”
HIV’s hidden DNA
Scientists have made some important discoveries about how HIV hides in the body that might lead them to develop new therapies.
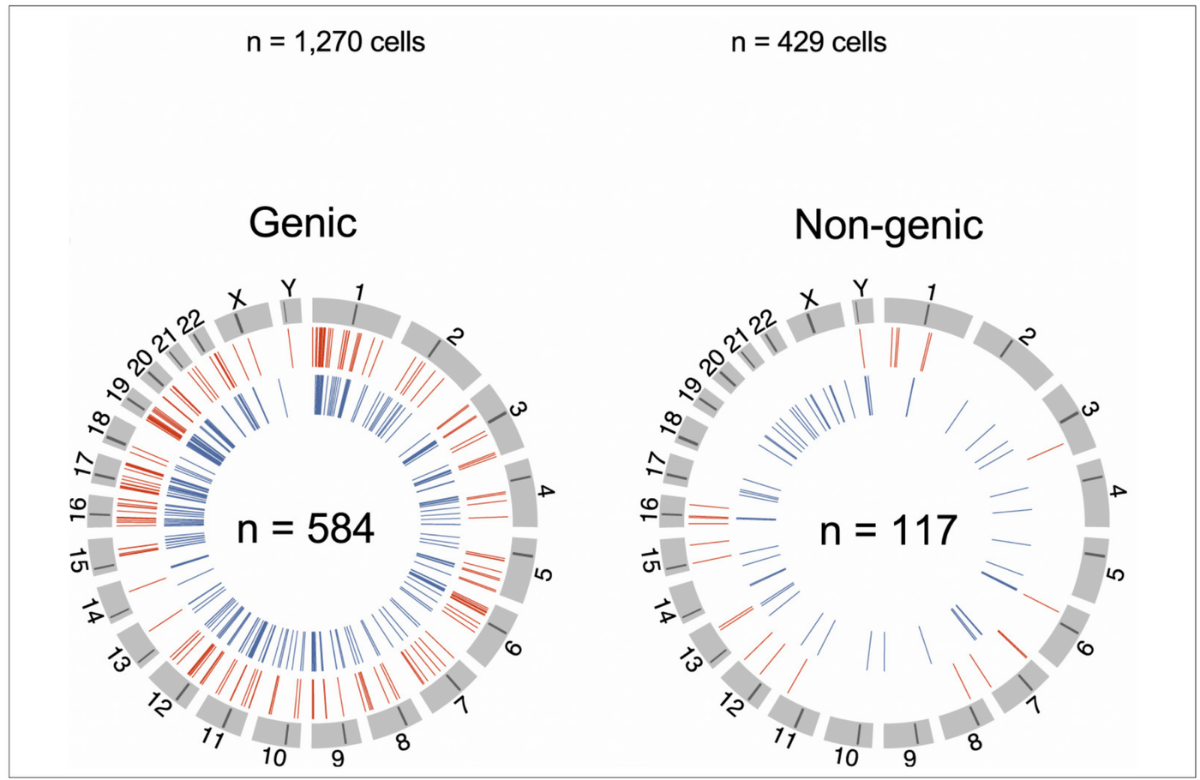
For the first time, they have mapped every piece of HIV proviral DNA hidden inside the genetic code of six people. They also charted exactly where the viral DNA was located within the participants' own DNA. This turns out to predict whether that particular piece of HIV can ever give rise to an infection again.
When people first acquire HIV, like other viruses it takes over cells and turns them into factories to make more virus. However, HIV has two tricks up its sleeve. Firstly, its preferred target is the very cells that should defend us against viral infections. Secondly, a proportion of those cells do what all immune cells do in a viral infection – they turn into long-lived memory cells, whose job is to recognise previous infections. (This is how vaccines work.)
As a retrovirus, HIV can insert its DNA into the DNA in our cells – and as some of those cells are memory cells, it stays there lifelong. If you remove the antiretroviral (ARV) drugs that jam the virus's copying mechanism, it comes flooding back.
A couple of years ago the same researchers took a look at what was going on in the one-in-200 people who do not need ARVs to stay undetectable – the ‘elite controllers’.
They found that, while elite controllers had less proviral DNA than non-controllers, more of it, surprisingly, was capable of being reassembled into whole viruses (a lot of proviral DNA is fragmentary).
However, more of the DNA was stranded in so-called ‘gene deserts’ – lengths of junk or structural DNA that are not capable of activating as genes.
The new study found the same thing had happened in four out of its six patients, who had been taking ARVs for nine to 15 years. The researchers hypothesise that the immune system can sense the very low-level HIV replication that is happening even in people on ARVs, and selectively kills off the cells that can still do this. The amount of low-key viral production of the molecule that’s evidence of this, messenger RNA (mRNA), was lower after years on ARVs.
In two people, mRNA production did not go down. In one, proviral DNA was found in the middle of a human gene that induces cells to divide. In the other, proviral DNA was sited very near a piece of DNA that was epigenetic – not a gene in itself, but a ‘switch’ that if turned on, causes nearby genes to activate.
The researchers suggest that in these patients the proviral DNA perpetuates, not by making new virus, but because the memory cells copy their DNA and divide – so the proviral DNA gets copied with them.
These findings point to two possible kinds of therapy that could enable more people to become controllers – one that sharpens the immune system’s sensing of viral mRNA and one that discourages memory cells from clonal division.
New edition of HIV & women

A new edition of our booklet HIV & women is now available.
Staff and patients at UK-based HIV and GUM clinics that are members of our subscription scheme can access the booklet on the clinic portal and clinics can order printed copies for delivery later this month.
To find out if your clinic is registered or for information on joining the scheme, please email us at info@nam.org.uk.
Chemsex

Fear of judgement is preventing gay and bisexual men from discussing chemsex with healthcare professionals, according to Australian researchers.
The researchers wanted to find out if men who have chemsex know where they can go for information, advice and support. They found that only a small proportion had discussed chemsex with any healthcare professional at all.
The men who took part in the study had got information about chemsex from friends (33%), casual sex partners (32%), LGBTI+ organisations (30%), sexual health doctors (28%), strangers on dating apps (26%), general practitioners (25%), the online community (25%), regular or romantic partners (23%), sexual health nurses (22%), general counsellors (17%), community health workers (15%), sexual health counsellors (13%) and non-LGBTI+ community organisations (9%).
More participants would feel comfortable talking to a sexual health doctor or sexual health counsellor than other healthcare professionals. Information received from sexual health doctors, LGBTI+ organisations and substance use organisations was perceived as more trustworthy and relevant than information from other sources.
Some LGBTI+ organisations and sexual health clinics already offer a lot of support around chemsex, but the researchers say that other services of this type have room for improvement.
HIV information in 25 languages
We want as many people as possible to have access to accurate, useful information about HIV in the language most useful to them.
In the Languages section of aidsmap.com, you'll find translations of our pages in 25 languages, including leaflets from The basics series, factsheets, booklets and conference bulletins.
If you or your organisation have translated an aidsmap page, share it with us and we’ll share it with everybody.
Editors' picks from other sources
HIV mRNA vaccine trial is now underway | POZ
The experimental HIV vaccine regimen aims to train B cells to produce broadly neutralising antibodies.
Zimbabwe: NAC discourages HIV supplements | AllAfrica
The National AIDS Council (NAC) has discouraged people who are on antiretroviral treatment from taking herbs or other drugs as cure for HIV and AIDS.
Shigella is an STI increasing among gay and bi men in the UK – but have you ever heard of it? | Gay Times
Shigella is a bacterium that causes a gut infection with symptoms ranging from feeling sick, severe diarrhoea, vomiting, abdominal pain, and fever. As symptoms are similar, it’s often mistaken for food poisoning.