Developing a common standard of HIV care throughout Europe, and an audit programme to monitor its implementation, needs to be developed more slowly than originally envisaged, owing partly to the difficulties of implementing it during the COVID epidemic. This was the outcome recommendation of a series of meetings convened by the European AIDS Clinical Society (EACS), the pan-European organisation of HIV physicians, that took place between last November and February. However, participants agreed that the success of a pilot audit has shown that a Europe-wide audit of certain guidelines is feasible, and the project remains on track over a longer timescale.
The Standard of Care for HIV & Coinfections in Europe, organised by EACS, is a long-term project aiming to set up a common, auditable standard of care for HIV throughout Europe.
The 2020 Standard of Care meeting had been planned for Tbilisi, Georgia, but it had to become a largely virtual one, due to COVID. It was split into five shorter meetings: an opening session, which took place in Tbilisi in October; three workshops; and a wrap-up meeting. You can download the full meeting report by aidsmap from the EACS website.
The workshops looked at:
- The effects of COVID-19 on health care throughout Europe, particularly with relevance to HIV services.
- The barriers to the delivery of PrEP in Europe, including the challenges and opportunities offered by the COVID epidemic.
- Proposals for the first substantive European audit, which is planned to cover co-morbidities in ageing patients with HIV.
The wrap-up meeting considered the proposals from the three workshops and outlined the way forward.
The opening meeting
The opening meeting heard how, for the first time, EACS, in collaboration with the European Centre for Disease Prevention and Control (ECDC) had conducted an audit of certain HIV clinical services, measuring provision in five disparate countries (Georgia, Germany, Poland, Romania and Spain) against one set of standards, and comparing the degree to which different countries and clinics met that standard.
Former British HIV Association (BHIVA) Chair Professor Jane Anderson said that audits are not research as such. Audits are quality improvement activities. They deal with the possibilities for improvement that exist in current healthcare settings.
Professor Chloe Orkin, immediate past BHIVA Chair, said that audits have to be relevant to existing guidelines, investigate systems that are already in place, and deal with simple data that are collected in standard practice. The annual BHIVA audit, which served as part of the template for the EACS pilot, started in 2001 and had focused on a large variety of different clinical priorities.
Final topics for an EACS audit would be decided by an expert group and audits conducted every one to two years. In some cases, it might be more realistic to measure local standards against other clinics or regional services in the same country.
The 2020 audit on viral hepatitis was a pilot project designed to demonstrate that such an exercise was possible. Modest in size and time frame, it was undertaken entirely in clinicians’ spare time and was processed manually; investment in an IT system would be necessary to enable a full-scale audit programme. Even so, it represents a considerable leap forward in a long-standing project.
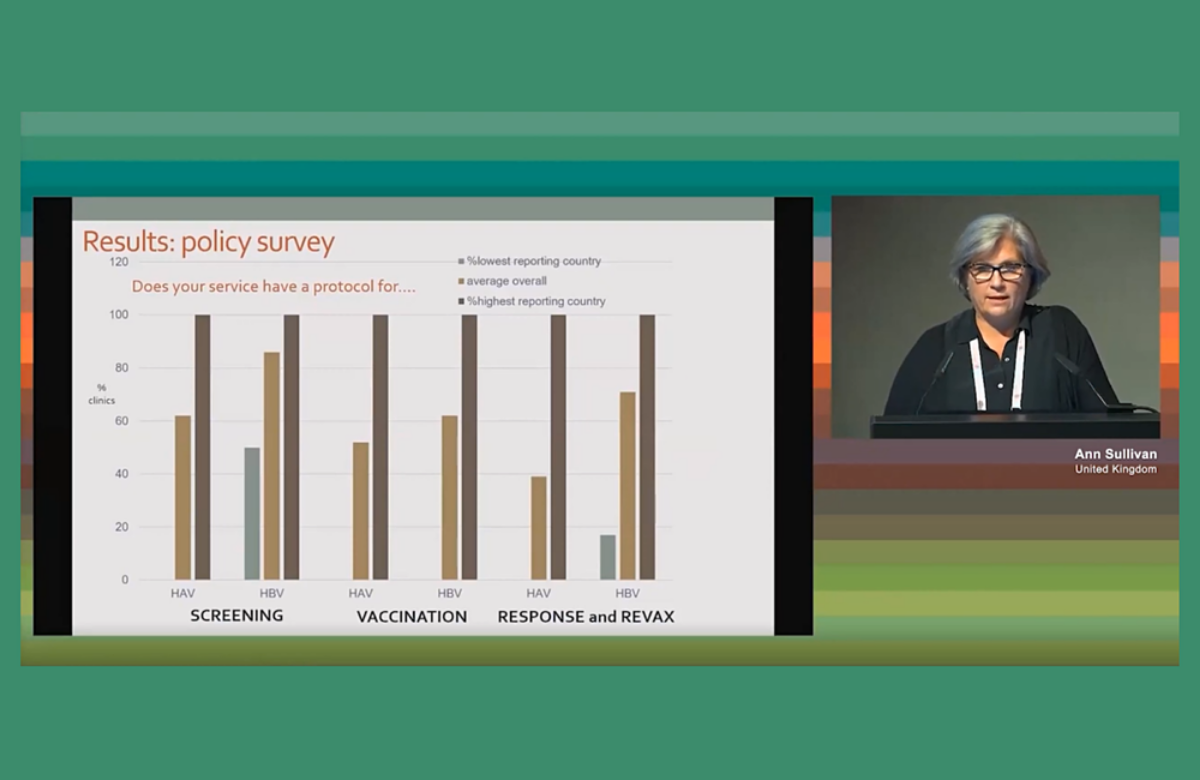
Dr Ann Sullivan of London’s Chelsea and Westminster Hospital presented the results. Amongst other things, it measured screening for hepatitis A, B and C viruses (HAV, HBV, HCV); hepatitis delta virus (HDV) in people with chronic hepatitis B; vaccination rates for hepatitis A and B; and the proportion of people with hepatitis C given direct-acting antiviral treatment.
There was wide variation between countries. In some, all services had protocols saying that all patients should be screened for HAV and HBV; at least one country did not have a policy of offering HAV screening at all. With HBV screening, most patients had had the hepatitis B surface antigen test, which indicates current infection. HAV screening was less consistent. While all patients in one country received an HAV screen, only 7% in another country and 36% in another had received one.
There was similar variability with HDV. No patients in one country had been screened for HDV, and no patients in two individual clinics each in two other countries had been screened. Since HBV/HDV co-infection is the condition with the most serious outcomes for viral hepatitis, Sullivan described these results as “disappointing”.
Vaccination rates for HAV and HBV were more challenging to interpret. In some countries, patients are referred to other services for HBV vaccination. In one country HBV vaccination was not reimbursed so had much lower rates. In contrast, there were encouraging rates of HCV treatment: 80% of co-infected HCV patients had received direct-acting antiviral treatment and it was planned for most of the other patients.
The COVID workshop

The COVID workshop took stock of the COVID situation throughout Europe and how it was impacting on HIV services. This workshop paid particular attention to the situation in central and eastern Europe, as its panel included HIV physicians from Czechia, Estonia, Poland and Romania, with a fifth from the UK.
Romania had been particularly badly hit. The healthcare system in Romania is inherited from the communist-era system which split hospitals into general ones and those catering for specialist conditions, including infectious diseases. To some extent this was also still the situation in Poland and Estonia.
Interestingly, COVID seems to have finally helped to enforce change in this system, with Poland introducing multidisciplinary, ‘multi-profile’ hospitals and four new ones being opened in Bucharest in Romania.
Despite different healthcare systems and levels of resources, the challenges COVID imposed on countries’ healthcare systems in general, and on healthcare services for people with HIV, were similar.
HIV services had been cut, with face-to-face appointments restricted to new diagnoses and people with severe health issues. As other surveys have shown, phone and video consultations, home testing, delivery of antiretrovirals, NGOs taking up some of the slack in services and other measures had between them been able to keep a basic level of services going. However, viral load monitoring in many countries had been reduced to at best once a year.
Quarantine or sheltering restrictions imposed on people with HIV had had the effect of deterring some from seeking medical help even when they needed it; when patients did start returning, the health of some had deteriorated.
The workshop recommended that testing all people hospitalised with COVID for HIV should be adopted by EACS as a Europe-wide policy. New HIV diagnoses had been found in patients admitted for COVID. The Bucharest clinic had found three new cases in 1200 COVID admissions. This rate of 0.25% is above the generally accepted threshold for the cost-effectiveness of HIV testing, which is 0.1%. Two of these patients were late diagnosed and one, who presented with COVID, HIV and multidrug-resistant TB, unfortunately died. In the UK, testing for HIV in patients admitted for COVID was incorporated early on after an unusual case in which one patient, apparently with COVID symptoms, when finally tested for HIV, turned out to have Pneumocystis pneumonia, not COVID.
The workshop considered setting minimum standards for HIV cases during the COVID epidemic, such as a certain frequency of monitoring, but a majority were concerned that setting out minimum standards might have the inadvertent effect of depreciating the Standard of Care that the existing EACS guidelines uphold.
The workshop also recommended an audit or look-back at the effect of COVID on HIV services and results conducted after the crisis had abated.
Although the agenda for the 2020 Standard of Care meeting was to do with keeping the momentum going towards achieving auditable standards, in the words of one doctor, “COVID was unprecedented, so there’s no previous standards to audit against. We can look back and analyse its effects, but there are no indicators to tell us that we could have done anything differently.”
The PrEP workshop
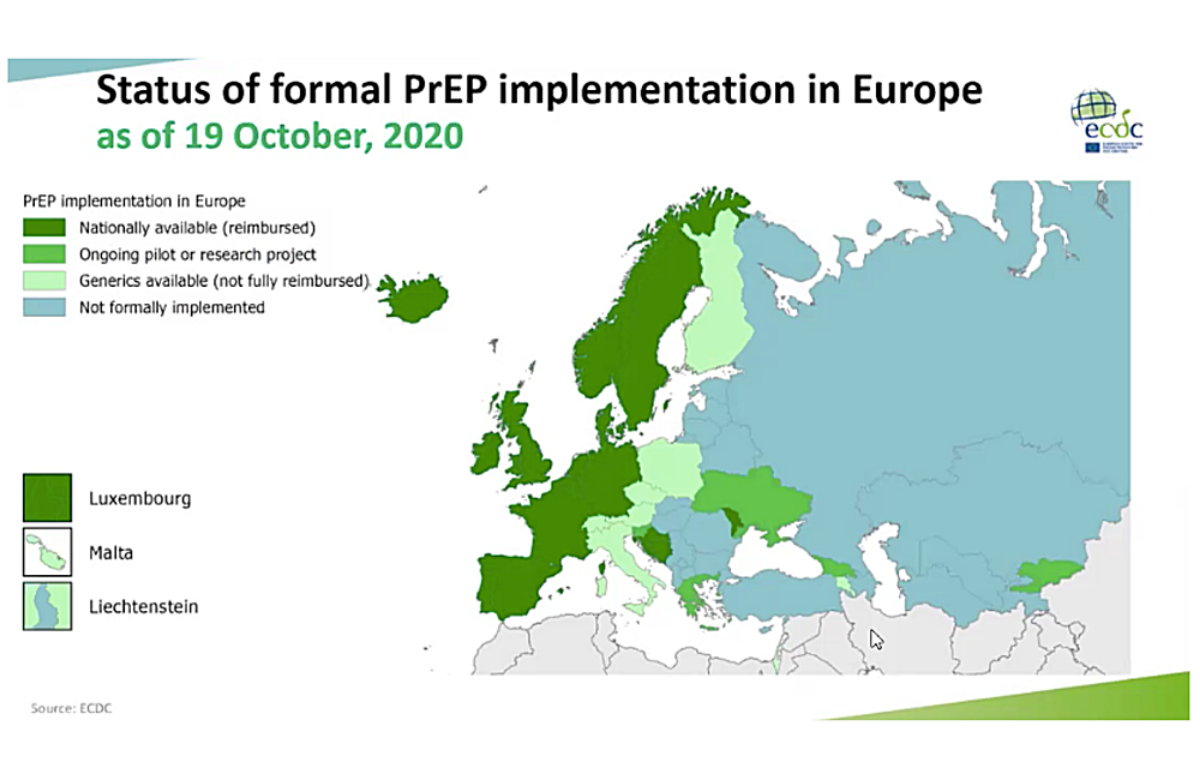
The PrEP workshop found that there remains a substantial gap throughout Europe between the need and desire for HIV pre-exposure prophylaxis (PrEP) and the number of people actually using it.
Twenty-eight European countries now provide some form of access to PrEP. This still leaves over 20 countries where there is still no systematic provision. But ECDC has calculated that the real gap in PrEP provision lies between the number of people who say in surveys that they would use it, and the number who actually do.
In the 2017 EMIS survey 21% of respondents in EU/EFTA countries said they would be “very likely” to use PrEP if they knew how to get it. However, only 3.2% actually used PrEP. Outside the EU/EFTA countries, in eastern Europe, the gap was bigger. It is estimated that half a million people in Europe would likely use PrEP if it was easily accessible.
There has been little research outside Africa to establish need in other populations such as women.
A community representative said: “With cisgender women especially, HIV may not be the first sexual health issue women think about, if at all. PrEP needs to be provided through gynaecological and family planning services to interest them in this additional sexual health protection mechanism.”
There was discussion about whether PrEP services could be ‘demedicalised’ to some extent without compromising safety. But there was concern about online purchases of PrEP drugs unlinked to medical monitoring. A better model might be what was called “a light-touch patient-controlled situation that gave PrEP users access to the tests they need.”
An NGO-based referral system might also help more people who are not gay and bisexual men to access PrEP. In Ukraine, there are currently 2269 people receiving PrEP. NGOs provide risk assessments and HIV testing, then refer those who are interested to a clinic. Of those referred so far, 17% are not gay men, including 128 female sex workers, 73 people who inject drugs and their partners, and 135 HIV-negative partners of people with HIV.
Within the English IMPACT trial, some sexual health clinics gave out a tick-box survey to all female attendees in the trial’s last month. It asked if there were any features in their lives that might indicate HIV risk such as unstable housing, intimate partner violence, or partners from high-prevalence countries. A ‘yes’ to any question triggered an HIV risk chat with a sexual health advisor. “We recruited as many women in that month as we did in the previous 18 months,” one doctor said.
There has been almost no research into intermittent PrEP regimens other than the 2-1-1 regimen used in the IPERGAY study. Research also needs to be conducted into the way people stop PrEP, and why.
ECDC has recently released its Operational Guidance on PrEP. This compares how PrEP provision works in different countries and sets down recommended procedures and standards. These could be used as the basis of an EACS/ECDC auditable Standard of Care on PrEP.
The audit workshop

The audit workshop looked at co-infections among people with HIV aged over 50 because this was suggested as an appropriate subject for the first general EACS audit. However, it ended up recognising that a number of factors made it difficult to move immediately to a pan-European audit structure.
Europe does not have an ‘audit culture’; the whole idea was novel to a number of the doctors who took part in the pilot. It took years for the BHIVA audit programme to become well-established enough for most HIV clinics in the UK to decide to devote the staff time necessary to do it.
The most sophisticated part of auditing is the setting of targets that are realistic enough to be achieved. Such targets should not set clinics up to fail, but should be high enough to serve as a challenge to improve services. Guidelines need to be auditable; that is, they need to be simple enough to be easily measured, apply to enough patients to generate meaningful data, and be capable of being presented in a numerically comparable way.
The EACS guidelines, while specifying a large number of procedures and standards, have not been critically analysed to see which can be and would profitably be the subject of auditable targets.
Europe’s variety of healthcare systems and of the demographics of its HIV-positive patients, narrows the potential number of pan-European targets.
Finally, there are practical matters. It will be hard to drive the audit programme forward in the middle of the COVID epidemic, when healthcare workers are redeployed and HIV-related activity during the last year will not be typical. The cost of staff time, data-processing software, and training, needs to be funded.
Because of these considerations, the workshop decided to recommend that EACS step back from setting up a European audit straight away and instead work with EACS’ existing Monitoring and Guidelines Group to establish a core auditable set of indicators, and to start initially by conducting in-country or possibly regional audits.
The wrap-up meeting

The wrap-up meeting in February heard summaries of all the workshops. It was accepted that the current situation made devising and conducting an audit in time for the next EACS conference this October difficult and that a two-year timescale was more realistic for the suggested work with the Monitoring and Guidelines Group to be done.
However, there was reaffirmation of the overall goal of a pan-European audit, at least of some services.
Professor Jürgen Rockstroh, President of EACS, said that he felt it was important for EACS to continue the momentum of the 2019 Bucharest meeting, which was the first in the Standard of Care series to result in a practical proposal which was then carried out. However, he said he could also see the point of ensuring that countries audit the outcomes that were of most relevance to them.
Dr Sanjay Bhagani, who will become EACS President after the October 2021 conference, said that the proposals of the audit group and from the other workshops would be considered by the EACS governing council and that the possibilities for funding such work would be actively explored.
Professor Michel Kazatchkine, former Director-General of UNAIDS and currently on the World Health Assembly body reviewing the global response to COVID, said that COVID had shown more than ever before that Europe was one region. Despite its variety of healthcare systems and economies, it had a strikingly similar pattern of the development of the COVID epidemic between west and east.
He also emphasised that COVID was likely to become a persisting health threat. New patterns of services, including for HIV, needed to be devised for this new world. In particular, he emphasised, some of the most innovative ways to maintain HIV services had come from NGOs; the importance of including civil society within health care as equal partners was more important than ever.