Europe losing ground on HIV targets as deaths rise
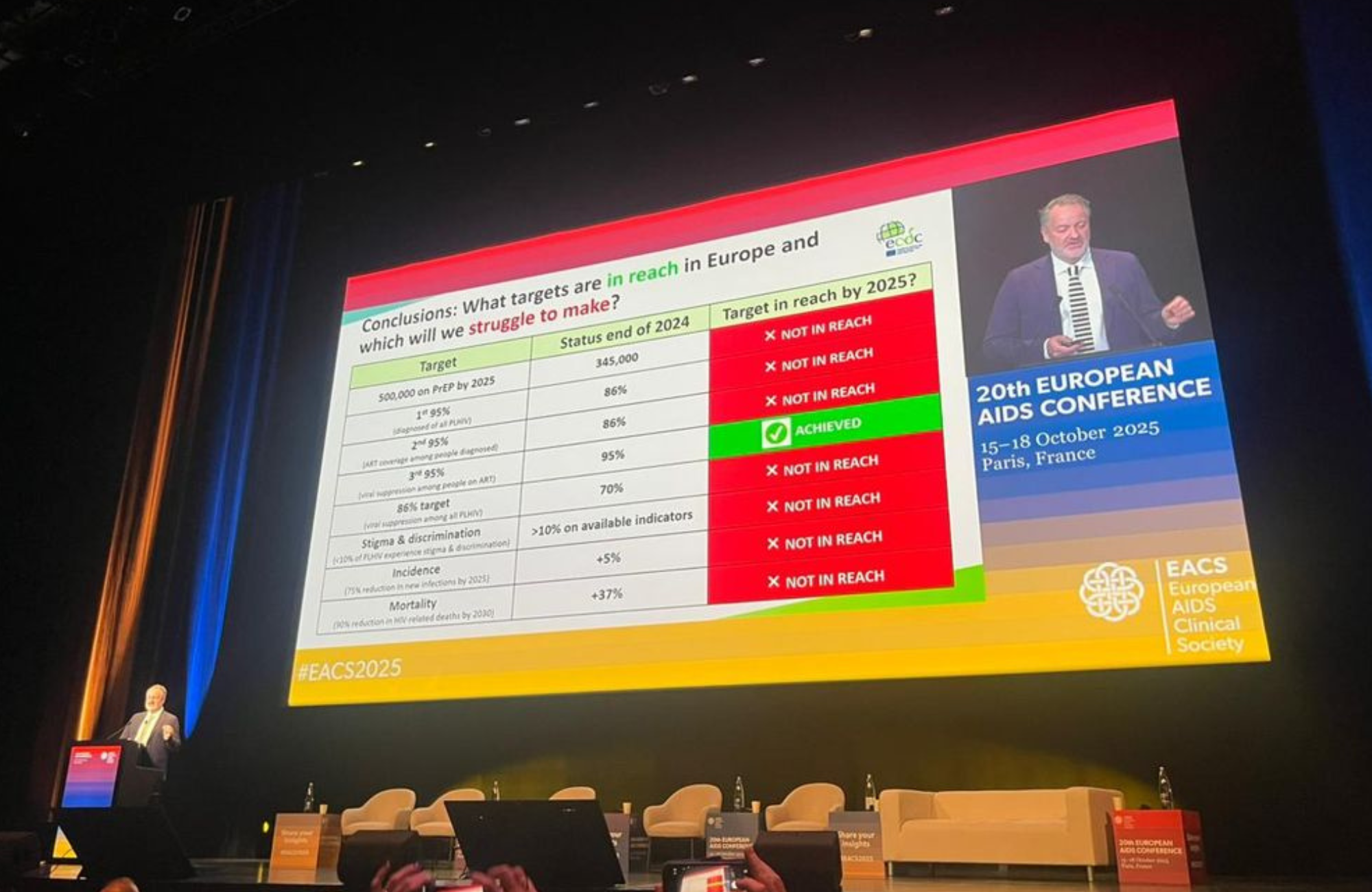
Europe is the only global region where HIV-related deaths increased between 2010 and 2022, the 20th European AIDS Conference (EACS 2025) heard in Paris. Teymur Noori of the European Centre for Disease Prevention and Control told delegates that Europe would miss most of the UNAIDS targets set for 2030, with war, funding cuts and political shifts deprioritising HIV as a global health issue.
The data paint a concerning picture. Whilst HIV-related deaths have halved globally since 2010, they have risen by a third in the WHO European region, which stretches from western Europe to central Asia. Deaths increased from 37,000 in 2010 to 51,000 in 2022 – more than five times the 2025 target. Many of these deaths are occurring in Russia and Ukraine. Even in wealthier EU and EEA countries, there were 2300 deaths in 2025, still more than twice the target.
The analysis reveals that approximately 30% of all people with HIV in Europe – around 620,000 people – live with transmissible levels of the virus. This is double the 95-95-95 target for 2030. Progress on viral suppression stalled when COVID-19 hit in 2020, with slower improvement since then. In eastern Europe, half of transmissible HIV is among undiagnosed people, while surprisingly, one-third of people with transmissible viral loads in western and central Europe are on treatment but not virally suppressed.
On the individual 95-95-95 targets, Europe has only achieved the third: 95% of people on treatment are virally suppressed. However, just 86% of people with HIV know their status, and only 71% of all people with HIV in the region are on treatment – below the global average of 77%.
PrEP provision remains deeply unequal. While 345,000 people have started PrEP, over 70% are in just four countries: the UK, France, Germany and Spain. Despite women potentially representing as many high-risk individuals as gay and bisexual men across the region, only in Ukraine are more than 10% of PrEP users female.
Noori acknowledged that "it was not all doom and gloom" with several countries making strides, but warned that "inequity in the provision of novel services pertaining to prevention, integrated testing, and gold-standard treatment is rampant across the European region."
Read this news story in full on aidsmap.com
New guidelines address breastfeeding, sleep and obesity

The European AIDS Clinical Society issued updated guidelines at the conference, making new recommendations on infant feeding and the diagnosis of obesity in people with HIV, as well as introducing routine screening for sleep disorders.
The revised infant feeding guidelines say that breastfeeding should be supported if women who are fully adherent and virally suppressed on continuous antiretroviral treatment want to breastfeed. The guidelines recommend that accessible, clear information relating to the very low but non-zero risk of transmission during breastfeeding should be provided to all pregnant women, ideally well before delivery, so that women can make a shared decision with their care providers. The guidelines clarify that mixed feeding with breast milk and solids raises the risk of HIV transmission and should be avoided, while mixed feeding with formula milk may be considered in specific circumstances. Monthly monitoring of maternal viral rebound is recommended, and breastfeeding should ideally be limited to no more than six months.
The guidelines recommend that doctors ask people with HIV "how is your sleep?" every two years, as well as after switching treatment. If patients report abnormal sleep patterns, more detailed screening should be carried out.
The updated guidelines incorporate a new definition of obesity, moving away from relying solely on body mass index (BMI) measurements. The authors emphasise that obesity is a condition caused by excess fat and that BMI measurements should be supplemented by measurements of total body fat by DEXA scan, or abdominal fat by waist circumference or waist-to-hip ratio. Individuals who have excess body fat but no organ dysfunction are considered to have subclinical obesity. Those with excess body fat and organ dysfunction have clinical obesity. Examples of relevant organ dysfunction include heart failure, atrial fibrillation, chronic knee or hip pain due to bearing excess weight, and substantial limitations of daily living.
The guidelines also make new recommendations on antiretroviral treatment for people who acquire HIV when using PrEP. Dual antiretroviral therapy regimens should be avoided, and boosted darunavir should be prescribed to people who were taking long-acting cabotegravir. The guidelines recommend an HIV viral load test before starting PrEP, especially if a high-risk exposure has taken place in the previous six weeks, whereas British and US federal guidelines do not require this.
Read this news story in full on aidsmap.com
Second Berlin patient's HIV cure linked to unusual immune response

The ‘second Berlin patient’ has been free of the virus for seven years after a stem cell transplant. He is the second person from Berlin (and the seventh globally) cured through this procedure. Researchers have now identified the remarkable immune mechanism behind his apparent cure: a potent antibody response working in conjunction with an unusual subset of his natural killer cells. Between them, they appear to have eliminated his HIV reservoir following his transplant for leukaemia in 2015.
Timo Trenkner from the University Medical Centre Hamburg-Eppendorf presented the findings at the conference. The research revealed that the patient's natural killer (NK) cells had high levels of a receptor called NKG2A⁺, which stimulated the production of antibodies exceptionally effective at neutralising HIV-infected cells. These antibodies outperformed broadly neutralising antibodies used in cure studies and those from elite controllers who naturally suppress HIV.
Professor Michaela Müller-Trutwin of the Institut Pasteur commented: "Although the antibodies generated by this patient were rather specific to his particular strain of HIV, they were very potent – better at neutralising infected cells than other broadly neutralising antibodies."
A crucial factor may have been that both patient and donor carried one copy of the delta-32 mutation, which made their cells partially resistant to HIV. This differs from most other cure cases, where donors had two copies of the mutation conferring complete resistance, while the donor to the ‘Geneva patient’ had no mutation at all. The patient's viral load had already declined from 13,000 to 1600 without treatment before his transplant. This lower viral load may have given his innate immune system the opportunity to mount an effective response.
"It looks like a high viral load overwhelms innate immunity," Müller-Trutwin explained. "But in people that may already have some, but not a lot, of virus in their blood, it may give the innate immune system a chance to mount an effective response."
Understanding how NK cells contributed to his cure could help develop safer, more widely applicable HIV cure strategies.
Read this news story in full on aidsmap.com
Quality of life in older people with HIV matches HIV-negative peers
A Dutch study comparing over 500 older people with HIV to matched HIV-negative controls found that whilst quality of life scores were slightly lower among those with HIV, the differences were too small to be clinically meaningful. However, people with HIV had significantly more symptoms of depression, exceeding the threshold suggesting clinical depression.
Kevin Moody of the University of Amsterdam Medical Centre presented findings from the AGEhIV cohort study, which tracked participants over eight years from age 52-53 to 60-61 on average. All participants completed the widely used SF-36 health-related quality of life questionnaire and the CES-D depression screening tool at baseline and at follow-up visits. The HIV-positive participants were all on antiretroviral therapy with viral loads below 200. Rather than comparing with the general population, researchers carefully matched them with HIV-negative people also attending healthcare facilities, particularly sexual health clinics, who had similar characteristics including co-morbidities, socioeconomic status and lifestyle factors. The majority of participants in both groups were White gay and bisexual men.
Quality of life scores were two points lower for physical activities and one point lower for mental tasks among people with HIV – differences that were statistically significant but, Moody noted, "of questionable clinical relevance". Encouragingly, scores barely changed over eight years despite participants ageing, with physical scores dropping by just one point regardless of HIV status.
Depression symptoms told a different story. Whilst scores remained stable over time, HIV-positive participants averaged 22.4 compared to 16.4 for HIV-negative participants. Those with HIV were around 50% more likely to report clinically relevant depressive symptoms.
However, general quality of life measures like SF-36 may not capture the psychological burden faced by people with HIV today. Moody emphasised that "targeted screening for specific mental health conditions, such as depression, may be more important for addressing psychological distress" than broader quality of life assessments.
Read this news story in full on aidsmap.com
Hepatitis B reactivation rare after switching from tenofovir-based HIV treatment
Two European studies show that hepatitis B reactivation is uncommon when people with HIV switch from tenofovir-containing regimens to alternative treatments, offering reassurance about newer HIV treatment options.
The issue has become clinically relevant as more people switch to two-drug regimens that don't contain tenofovir, a drug that also suppresses hepatitis B. Around 30% of people with HIV have evidence of past hepatitis B exposure (shown by antibodies to hepatitis B core protein (anti-HBc)), raising concerns about whether removing tenofovir might allow the virus to reactivate, potentially leading to serious consequences if undetected, including liver inflammation, cirrhosis, or liver cancer.
The Swiss HIV Cohort Study compared 197 people switching from tenofovir-containing regimens to those containing other hepatitis B-suppressive drugs (emtricitabine or lamivudine) with 197 who switched to regimens without these drugs. During median follow-up of 1.3 years, 5.6% of those on regimens without hepatitis B activity showed signs of reactivation compared to 1.1% of those with some protection. However, all cases were mild – hepatitis B DNA remained below quantifiable levels and none tested positive for active infection markers.
A study of 741 people in Barcelona switching to injectable cabotegravir/rilpivirine found that only two participants experienced hepatitis B reactivation. Both had undiagnosed chronic infection at the time of switching, and both were successfully re-suppressed after resuming tenofovir-based treatment.
"We believe that our findings are reassuring for persons with HIV and positive anti-HBc and their physicians that switching to a non-tenofovir-based ART is possible," concluded Dr Lorin Begré of Bern University Hospital.
Experts agreed that while reactivation risk is extremely low, proper counselling and hepatitis B vaccination remain essential for people with past exposure.
Read this news story in full on aidsmap.com
Ukraine harnesses AI to sustain HIV services during wartime

Ukrainian health services are deploying artificial intelligence (AI) in innovative ways to maintain HIV prevention and care despite the ongoing conflict. Tetiana Deshko of the Alliance for Public Health described three applications at the European AIDS Conference in Paris: chatbots using animated avatars, machine learning to improve HIV testing efficiency, and AI-assisted crisis planning.
The chatbot TWIIN uses 'digital humans' – interactive avatars based on real community health workers and service users – to answer questions about sexual health, drug use and HIV services for key populations. These embodied agents create stronger emotional connections and have greater impact on health behaviours than text-based services, Deshko said. In the last quarter of 2024, TWIIN reached 4702 people with information on topics including PrEP, PEP, overdose prevention, opioid substitution therapy and chemsex. The chatbot directs users to a telehealth platform where they can order prevention supplies, arrange guided self-testing or schedule consultations with a doctor.
The Alliance is also using machine learning to identify which newly diagnosed people are most likely to recruit peers for HIV testing through their social networks. While health workers initially selected people to receive coupons and incentives to encourage testing among their peers, AI analysis can detect risk factors that humans might miss, especially in contexts of population displacement which may change the local epidemiology. In 2024, the 55 cases selected with machine learning support recruited 922 peers for testing, with a diagnostic yield of 5.6%. This compared favourably to the 4.3% yield when 67 cases were selected by staff, who recruited 3208 peers.
Finally, the organisation is using an AI conversational agent to help achieve ISO 22301 certification for business continuity management. This matters because the Alliance must be prepared to maintain service delivery and protect client data during crises such as cyberattacks, bombing and infrastructure failures. The AI assists with analysing critical processes, dependencies and risks, creating emergency plans, predicting potential disruptions and providing real-time decision support during incidents. Deshko said this makes business continuity management accessible even to organisations with limited resources.
Read this news story in full on aidsmap.com
Early and aggressive cases of prostate cancer in men with HIV
Men with HIV are diagnosed with prostate cancer a decade earlier than the general population and appear to be more likely to have advanced disease at diagnosis, according to a German study presented at EACS 2025. The findings suggest that men with HIV may benefit from screening to catch prostate cancer before it spreads.
The study included 161 men with HIV diagnosed with prostate cancer across 16 HIV clinics. Diagnosis occurred at a median age of 61 years, compared to 71 years in the general German population. At diagnosis, over a quarter (26%) already had metastatic disease that had spread beyond the prostate, 59% had cancer assessed as high risk of progression, and the average PSA level was substantially elevated at 17ng/ml.
Men with CD4 counts below 500 were significantly more likely to be diagnosed with metastatic prostate cancer. While overall survival was poorer in men who received radiotherapy compared to other treatments, only one death was directly attributable to prostate cancer.
Based on these findings, the German investigators recommend PSA screening should begin at age 45 in men with HIV, aligning with new German national guidelines.
Other studies at the conference highlighted additional cancer screening gaps. Women with HIV in Italy often don't perceive themselves at risk of anal cancer despite high prevalence of HPV strains associated with cancer, with 45% refusing screening. Based on the incidence of cervical cancer in the Netherlands over two decades, researchers concluded that cervical cancer screening should prioritise younger, newly diagnosed women with low CD4 counts and those recently virally suppressed.
Meanwhile, a three-country study found hepatocellular carcinoma (liver cancer) screening remains underutilised in people with HIV and hepatitis B co-infection, particularly among those without cirrhosis – only 24% of eligible individuals without cirrhosis were screened despite many having risk factors.
Read this news story on aidsmap.com
Injectable HIV treatment failures can limit future drug options

When the long-acting injectable HIV treatment cabotegravir/rilpivirine fails, more than half of people develop resistance to multiple drug classes, potentially limiting their future treatment options, Dr Maria Mazzitelli of Rome Catholic University reported at the conference.
The researchers reviewed all published cases of virological failure on cabotegravir/rilpivirine that included resistance data. They identified 94 cases representing 1.3% of people who started the injectable treatment in the reported populations. The researchers assessed the resistance mutations detected against data on viral sensitivity to other integrase inhibitors and non-nucleoside reverse transcriptase inhibitors (NNRTIs).
Among 45 cases with full information on known risk factors for failure – high body mass index, baseline rilpivirine resistance mutations, or specific HIV subtypes – 57% had no risk factors and 37% had one. Low drug concentrations were found in 29% of cases tested, but this didn't differ from people who remained virally suppressed, suggesting drug levels alone couldn't explain treatment failure.
Resistance testing after virological failure revealed that 56% had resistance to both rilpivirine and cabotegravir, 27% had reduced susceptibility to rilpivirine alone, and 5% to cabotegravir alone. Using the Stanford resistance database, the investigators estimated that 44% would have reduced susceptibility to the integrase inhibitors dolutegravir and bictegravir, 39% to the NNRTI etravirine, and 35% to the NNRTI doravirine. However, high-level resistance was less common, suggesting that second-generation integrase inhibitors could still be used in combination with other fully active agents in most cases.
A separate meta-analysis of seven clinical trials presented at the conference reinforced concerns about resistance development. Although virological failure rates were similar in people taking cabotegravir/rilpivirine or three-drug oral regimens containing dolutegravir, 67% of people experiencing failure of cabotegravir/rilpivirine developed integrase inhibitor resistance mutations compared to none taking dolutegravir-based oral regimens. This represented a fivefold higher risk of developing integrase inhibitor resistance.
The findings highlight the importance of careful monitoring and prompt action when viral rebound occurs on long-acting injectable treatment.
Read this news story in full on aidsmap.com
More news from EACS 2025

Chemsex use is changing in Europe
The way gay and bisexual men are using drugs to enhance sex (chemsex) is changing in Europe, especially among younger men and those new to chemsex. They are turning to a new generation of drugs, generally with shorter half-lives. These include synthetic cathinones similar to mephedrone, but there are signs that hallucinogens like LSD are also regaining popularity.
Increased STI diagnoses in gay men with HIV are mainly due to more testing
A study presented at EACS 2025 has found that the apparent rise in sexually transmitted infections (STIs), at least in gay and bisexual men with HIV in France, are due to more frequent testing rather than more infections. Dr Sophie Novelli presented data from 2016 to 2023 taken from the PRIMO cohort.
STIs and doxyPEP at EACS: community effectiveness, gonorrhoea resistance and ‘blunted’ syphilis
A significant number of presentations at EACS 2025 were concerned with the bacterial sexually transmitted infections (STIs) syphilis, gonorrhoea and chlamydia rather than HIV. This is largely because using the antibiotic doxycycline to forestall infection after possible exposures – doxyPEP – has become more common in western Europe.
Less weight gain with Dovato than Biktarvy
Switching to a two-drug regimen of dolutegravir / lamivudine (Dovato) resulted in significantly less weight gain after 96 weeks compared to a switch to tenofovir alafenamide / emtricitabine / bictegravir (Biktarvy), the final results of a large, randomised trial conducted in Spain have shown. Dr Esteban Martinez presented 96-week results of the PASO-DOBLE study.
Too few people with HIV receiving statins despite guideline changes
Progress towards wider use of statins in people with HIV has been modest and LDL cholesterol control remains suboptimal in people with HIV at higher risk of cardiovascular disease, studies presented show.
Updated About HIV pages

We've been reviewing our About HIV information pages over the last few months. Our recently updated pages include:
- Menstrual health and HIV
- Sleep and HIV
- Alcohol and HIV
- The stages of HIV infection
- What are the side effects of Truvada used as PrEP?
Editors' picks from other sources
With community health workers fired, who's on the frontline? | Forsaken
The Trump administration spent months eliminating community health worker programmes. Now officials recognise their importance.
Breakthrough HIV prevention jab given green light in South Africa | Spotlight
An HIV prevention jab that provides six months of protection at a time was given the green light by South Africa’s medicines regulator. The approval helps to clear the way for a limited public sector rollout of the “game-changing” shot set to start in April 2026.
Local transmission of clade 1b mpox cases detected in EU/EEA, ECDC urges renewed vigilance | European Centre for Disease Prevention and Control (ECDC)
Following the first detections of locally acquired mpox clade Ib cases within the European Union and European Economic Area (EU/EEA), we are calling for heightened awareness and targeted prevention measures.
UNAIDS is set to close in 2026 – four years early. Are experts right to be alarmed? | The Guardian
The move to shut the agency comes as aid budgets are being slashed, leading to fears that global progress on HIV may be reversed.
NICE approves annual access to injectable cabotegravir PrEP in England for 1000 people | i-Base
NICE announced that long-acting cabotegravir injections (CAB-LA) will be approved as PrEP for a limited number of people in England who are not able to use oral PrEP.
Subscribe to aidsmap bulletins
Has this bulletin been forwarded to you? Sign up to aidsmap email bulletins to keep you up to date with the latest research, news and developments in HIV.