New EACS guidelines

Catia Marzolini, co-ordinator of the guidelines’ new drug interactions section, at EACS 2019. Image: Gus Cairns
The tenth edition of the European AIDS Clinical Society Guidelines was launched at the society's 17th European AIDS Conference (EACS 2019) in Basel, Switzerland last week. The new edition is more than twice the length of the previous version, which is evidence of the complexity of needs it seeks to address. In particular, as the average age of people with HIV increases, much of its new material has been developed with the needs of the ageing person with HIV in mind.
An important new section covers drug-drug interactions, addressing risky combinations with medications used to treat common co-morbidities, including statins, antidepressants and tuberculosis therapies. It includes a comprehensive guide to the dose-adjustment of antiretrovirals for people with kidney problems and a list of the top ten drug classes to avoid in older people living with HIV.
For the first time transgender people with HIV are catered for, with information on dose adjustments that may be needed for gender affirming hormones when combined with particular antiretrovirals.
The guidelines for recommended first-line antiretroviral regimens concentrate on what is likely to be the most tolerable and resistance-proof regimen. They generally recommend two nucleoside reverse transcriptase inhibitors plus a non-boosted, once-daily integrase inhibitor with a high genetic barrier to resistance – which in practice means dolutegravir or bictegravir.
A dual-therapy option is included for the first time – dolutegravir plus lamivudine. This should only be given to people with a baseline viral load below 500,000 and a CD4 cell count above 200.
The guidelines also include a clear statement supporting ‘undetectable = untransmittable’ (U=U), including how this information affects options for conception for people living with HIV and their partners.
Almost no cases of anal cancer in Australian study

David Templeton of the Study for the Prevention of Anal Cancer at EACS 2019. Image: Gus Cairns
An Australian study of 617 gay and bisexual men recruited in community settings in Sydney, Australia has found a very high prevalence of HSIL (high-grade squamous intraepithelial lesions – precancerous changes in the cells of the anal lining that may indicate a risk of developing cancer). At baseline, 32% of HIV-negative men and 47% of HIV-positive men had HSIL, Dr David Templeton told the conference.
However, after three years of follow-up, only one man out of 617 progressed to anal cancer. It is very difficult to calculate a population incidence from one case but this does seem to be out of line with the very high incidence rates quoted for HIV-positive gay men in previous studies.
The researchers also found that the incidence of new anal lesions was no higher in smokers and not much higher in men with HIV, both groups that are usually thought to be at higher risk.
Another encouraging finding was that clearance of HSIL – its regression either to normal cells or to a lower grade of abnormality – was more common than its appearance. Twenty-two per cent of men cleared their HSIL per year compared with 11% who developed it.
First European study of PrEP persistence

Dominique Costagliola of Inserm at EACS 2019. Image: Gus Cairns
PREVENIR, the French open-label study looking at PrEP use in gay and bisexual men in the Paris region, has found that 16% of study participants stopped taking PrEP within a year, and that 32% had discontinued PrEP after 30 months.
This is a higher rate of PrEP ‘persistence’ than has been observed in previous studies in the US. This is the first European study to report on the issue.
Most men who discontinued simply dropped out of the study rather than telling clinicians that they were stopping PrEP. When they did discuss it with staff, three-quarters said they no longer felt at risk.
Younger men (aged 25 and under), people with poorer education and men who had never taken PrEP before were all more likely to discontinue PrEP than other study participants. Financial status made no difference to PrEP persistence.
Dr Dominique Costagliola of the French health research institute Inserm told the conference that qualitative research focusing on young men who have sex with men with limited education could help, to understand the reasons they stop PrEP and to design targeted interventions aiming at increasing PrEP persistence.
Greatest weight gain in switching studies seen in black women

However, black people and women were most likely to experience substantial weight gain. The findings suggest that looking at averages in switch studies may be less useful than looking at risk factors for clinically relevant weight gain of greater than 5kg. This is especially the case in study cohorts such as these that are predominantly white and male.
Investigators from the AGEhIV cohort in the Netherlands designed a prospective observational study in which changes in body weight were monitored in people who switched to an integrase inhibitor-containing regimen. Each person was matched with two HIV-positive people who remained on non-integrase inhibitor treatment and two HIV-negative people.
Throughout the follow-up period there was no significant difference in body weight changes between people who switched to an integrase inhibitor-containing regimen (0.17kg a year) and matched HIV-positive (0.22kg a year) and HIV-negative controls (0.18kg a year).
But weight gain of 10% or more after switching occurred more frequently in black women than in other demographic groups, although there were not many black women in the cohort.
An analysis of 2186 people in the Swiss HIV Cohort Study who switched to dolutegravir found that they gained a median of 0.5kg in the 18 months preceding the switch, increasing to 0.7kg in the 18 months after switching.
When the researchers calculated the risk of gaining more than 5% in body weight after switching, they found that women, black people and current smokers had an approximately 50% greater likelihood of substantial weight gain.
A possible mechanism for weight gain on integrase inhibitors
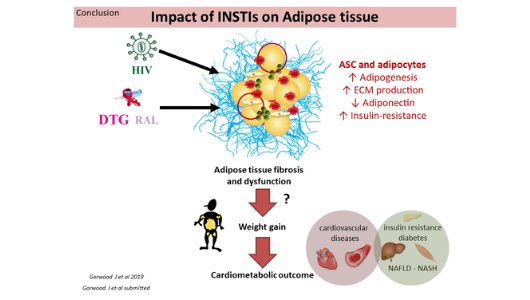
Slide from Jennifer Gorwood’s presentation at EACS 2019.
The integrase inhibitors dolutegravir (Tivicay, also in Triumeq and Dovato) and raltegravir (Isentress) cause changes in the structure of fat cells that may promote obesity and insulin resistance, Jennifer Gorwood of the Saint Antoine Research Centre, Sorbonne University, Paris told the conference.
Data come from studies of cells sampled from people living with HIV and monkeys exposed to the drugs. The findings suggest fibrosis in subcutaneous and visceral fat tissue after use of the integrase inhibitors, including peri-adipocyte fibrosis, which is associated with metabolic syndrome.
However, opinions vary among metabolic researchers regarding the significance of adipocyte fibrosis. These findings are preliminary and suggestive of further avenues for research rather than proof of a mechanism by which integrase inhibitors cause weight gain.